EPISODE 3
Key aspects of
diagnostics in asthma:
the Finnish perspective
INTRODUCTION
The Finnish Asthma Programme emphasised early diagnosis of asthma to enable timely initiation of treatment. Furthermore, it was believed that the diagnosis of asthma should be based not only on symptoms, but also on confirmed variable airflow limitations measured with objective lung function assessments, such as spirometry.
In the video interview, Professors Lauri Lehtimäki and Mika Mäkelä explore asthma diagnostics in Finland. Discover the basic principles and learn how to steer clear of common pitfalls. Gain more insights into the diagnostic procedures in use in Finland by exploring the text below.

Key aspects of diagnostics in asthma: the Finnish perspective
Understanding asthma as an inflammatory disorder, which can be detected early and treated effectively, was one of the basic principles driving the Finnish Asthma Programme. One of the goals of the program was to facilitate the recovery of as many patients with early asthma as possible. The first step for achieving this was efficient asthma diagnostics. (1)
One of the pivotal actions undertaken during the Finnish Asthma Programme involved the transition of asthma diagnostics from secondary to primary healthcare. After the transition, the primary responsibility for diagnosing asthma in adults shifted to general practitioners, while a respiratory physician was consulted only in cases requiring further examinations or when symptoms were severe. The diagnosis of asthma in children under 12 years of age was predominantly carried out by specialists. (2)
Objective lung function measurements: the cornerstone of asthma diagnostics
Asthma can be suspected if a patient has typical symptoms such as wheeze, chest tightness, prolonged cough, and sputum production. The probability of diagnosing asthma is increased by onset of symptoms in childhood, a history of allergic rhinitis or eczema, and a family history of asthma and allergies. The cornerstone of asthma diagnosis, however, is a confirmed variable and reversible airflow limitation. This means that the patient’s expiratory lung function varies over time and in intensity, and that the limited airflow may resolve spontaneously or in response to bronchodilators. (3) In Finland, this is part of the diagnostic criteria for asthma. Airflow limitation can be documented by measuring the forced expiratory volume in one second (FEV1) by spirometry or by measuring peak expiratory flow (PEF) (Figure 1). (4)
Professor Lehtimäki elaborated on the Finnish practice of conducting PEF measurements at home: “I think the only slight difference to international guidelines is in the way that we do PEF monitoring at home. It's for two weeks, triplicate measurements in the morning and in the evening, before and after bronchodilators.”
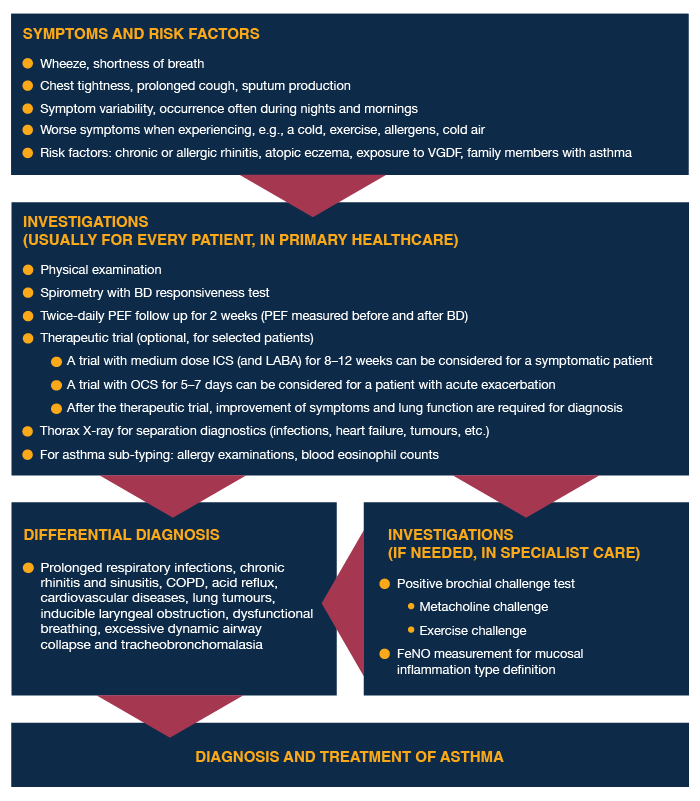
Figure 1. A simplified schematic view of asthma diagnostics in adults based on the Finnish Current Care Guidelines (4). BD, bronchodilator; COPD, chronic obstructive pulmonary disease; FeNO, exhaled nitric oxide; ICS, inhaled corticosteroids; LABA, long-acting beta-2-agonists; OCS, oral corticosteroids; PEF, peak expiratory flow; VGDF, vapours, gases, dusts, and fumes.
Special considerations of asthma diagnostics in children
Recurrent wheezing, a history of allergic disease, and a family history of allergy or asthma are the most important cues to suspect asthma in young children. (4) Professor and paediatrician Mika Mäkelä explained the importance of objective lung function measurements in the asthma diagnostics also in children: “Relying solely on symptoms for diagnosing asthma can lead to significant overdiagnosis and overuse of asthma medication."
According to Mäkelä, the Finnish guidelines for childhood asthma employ a three-step age-wise approach in diagnostics. In children under the age of three, one may have to rely on asthma predictive index, whereas in children aged three to seven, lung function measurements have proven to be a reliable method for distinguishing between asthmatic and healthy individuals. Lung function measurement methods available for children include impulse oscillometry, spirometry, field running test, and PEF measurements.
Did the Finnish Asthma Programme reach its goal of improving recovery of early asthma?
The patients in the Helsinki region reported significantly less asthma symptoms in 2016 compared to 1996 (p<0.05). (5) Many patients who previously received asthma medication reimbursement for a restricted period may no longer need it after successful initial treatment, indicating recovery. (1)
Overall, a crucial aspect of asthma diagnostics is the confirmation of the diagnosis through objective lung function measurements, which applies to both adults and children. By incorporating objective measurements, such as lung function numbers, healthcare professionals can provide additional motivation for patients to actively treat their asthma.
You might be interested in these:
References
3. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2023. Available from: www.ginasthma.org.
4. Asthma. Current Care Guidelines. Working group set up by the Finnish Medical Society Duodecim, the Finnish Respiratory Society, Finnish Paediatric Society, and Finnish Society of Clinical Physiology. [Internet]. Helsinki: Finnish Medical Society Duodecim; 2022 [cited 2023 Apr 19]. Available from: www.kaypahoito.fi
RESP-1483c 05/2023