Three facts about MART - check your knowledge
Insights | 29/10/2025
- MART has been established as the preferred option for asthma management in international guidelines.1
- This approach utilises the same inhaler for daily maintenance and reliever therapy.1,2
- The combination of ICS-formoterol offers several benefits over a separate SABA reliever.1,2
MART is the preferred treatment option for asthma patients in need of both daily maintenance and quick relief. MART inhalers combine two medications with different mechanisms of action. An inhaled corticosteroid (ICS) such as budesonide addresses the root cause of asthma by reducing inflammation in the airways. ICS-containing treatment is recommended for all patients aged 6 and older to reduce severe exacerbations and control symptoms. A bronchodilator (formoterol) opens the airways and provides fast symptom relief. This combination provides both maintenance (daily use) and reliever (as-needed) therapy in a single inhaler.1,2
Read on to learn more about MART and its benefits:
Fact 1: Formoterol acts as fast as salbutamol
There may be uncertainty about how formoterol compares to salbutamol, which has been the standard reliever therapy for decades. Both formoterol and salbutamol are rapidly acting β2-bronchodilators that provide quick relief of airway constriction. While salbutamol is short-acting, formoterol has a longer duration of action with an equally fast onset — within 3 minutes bronchodilation achieved with formoterol is comparable to that of salbutamol.3,4,5 This makes formoterol, when combined with an ICS, suitable for both maintenance and reliever therapy.
The combination of formoterol with an ICS maintains similar reliever efficacy while reducing the risk of severe exacerbations, as compared to SABA (short-acting β2-agonist) reliever therapy.1,2,6
Fact 2: Patients do not need an additional reliever inhaler when on MART regime
Working as fast as salbutamol to relieve symptoms, formoterol eliminates the need for a separate SABA inhaler. Using one inhaler for both maintenance and relief simplifies treatment and may help patients stay consistent with their medication.1,2 For patients unsure about moving to a MART regimen, consider allowing them to keep a SABA inhaler available for reassurance until their next review.
Note that ICS combinations with non-formoterol LABAs (long-acting beta-2 agonists) are not indicated for MART therapy due to a slower onset of action (e.g., ICS-salmeterol) or a lack of safety and/or efficacy with more than once-daily use (e.g., ICS-vilanterol, ICS-indacaterol). In these cases, an additional inhaler for reliever medication is needed. The use of multiple inhaler types should be avoided when possible, to avoid confusion.1
Fact 3: ICSs and LABAs work together to effectively control asthma
The combination of an ICS and a LABA has a positive effect that is particularly beneficial for asthma treatment. ICSs increase the number and sensitivity of β2-receptors, the target structure for LABAs in the airways. This helps enhance the effectiveness of LABAs.7 Additionally, LABAs can amplify the anti-inflammatory effects of ICSs by stabilizing cell membranes and inhibiting the release of inflammatory mediators.7 This mutual enhancement leads to effective control of asthma symptoms, reducing the risk of severe exacerbations.1,7
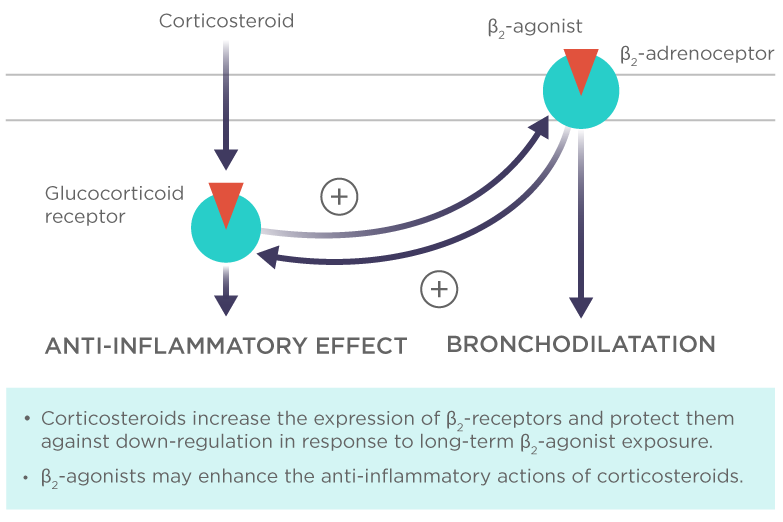
Figure 1. The interaction of corticosteroids and β2-agonists. Each class of drugs enhances the others beneficial actions. The figure has been adapted from Barnes 2002.
By understanding and utilizing MART therapy, patients can achieve asthma control and improve their quality of life.1 Stay informed to help your patients take charge of their asthma management!
References
- The Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention 2024. Available at: ginasthma.org.
- Beasley R, et al. J Allergy Clin Immunol Pract. 2023 Mar;11(3):762-772.e1. https://doi.org/10.1016/j.jaip.2023.01.002
- Bufomix (budesonide/formoterol) Easyhaler 80/4.5 and 160/4.5mcg SmPC, Orion Pharma.
- GSK. Ventoline® Evohaler® 100 µg. SPC.
- Jonkers RE, et al. Respir Res. 2006 Dec 4;7(1):141. doi: 10.1186/1465-9921-7-141.
- Kuna P, et al. Int J Clin Pract. 2007 May;61(5):725-36. doi: 10.1111/j.1742-1241.2007.01338.x
- Barnes PJ. Eur Respir J 2002;19:182−191. doi: 10.1183/09031936.02.00283202.
October 2025 / EASYH-4696
Was this article useful?
DATE OF PREPARATION: APRIL 2025/EASYH-688(11)
FULL PRESCRIBING INFORMATION AVAILABLE HERE
For more information about Orion and Sustainability click here
| Adverse effects should be reported. You can report side effects directly via the Health Products Regulatory Authority (HPRA) website: www.hpra.ie or by email on medsafety@hpra.ie. Adverse effects should also be reported to Orion Pharma via ie.medicalinformation@orionpharma.com |
